
Summary:
- Purpose: to summarize prevalence and etiology of accessory roots and root canals in anterior teeth, clinical and radiographical detection by conventional and contemporary tools, and treatment modifications and clinical outcome.
- Materials/Methods:
- Electronic search for articles published in Jan. 1970 to Nov. 2014 in 5 major endodontic journals; Australian Endodontic Journals, Dental Traumatology; International Endodontic Journal, Journal of Endodontics, and Oral Surgery Oral Medicine Oral Pathology.
- N: 86 Inclusion criteria; exclusion criteria: Table.1
Highlights:
- Maxillary anterior teeth: Most common root canal configuration is type IV (2-2) mostly in M-D direction.
- Mandibular anterior teeth: More complex and higher prevalence in accessory root/root canal variations/configuration than their maxillary counterparts. However, maxillary incisor revealed the highest tendency for accessory root/root canal aberrations caused by anomalies such as dens invaginatus and palato-gingival groove.
- Most common root canal configuration is type IV (2-2) and type V (1-2) mostly in labiolingual direction
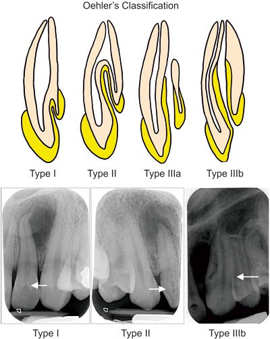
- Dense invaginatus:
- invagination of the enamel organ into the dental papilla prior to calcification Prevalence:ranges from 1% to 26%
- Types: Found mostly maxillary lateral > maxillary central > mandibular incisors and canine
- 1- Type I: (Most common); confined enamel form to the crown and do not extend to the CEJ
- 2- Type II: Confined enamel form extend to the root as a blind sac ± pulp communication. Radiographic appearance is a RL tear drop shape surrounded by RO border
- 3- Type III: The invagination perforate the root showing a second foramen; cementum is frequently found; no immediate communication to the pulp. Radiographic appearance is a blunderbuss opening to the PDL (pseudo canal).
- Palato-gingival groove (radicular lingual groove; disto-lingual groove):
- Prevalence: ranges from <1% to >18%
- Primary maxillary canine has more prevalence of Double roots than their mandibular counterparts
- Preoperative interpretation: Good quality preoperative periapical radiographs with more than one horizontal projection aid in accurately detecting root canal bifurcations and outline of the periodontal ligament.
- Postoperative assessment: Filling material (root canal sealer and thermoplasticized gutta-percha if applied) can propagate from the filled canal into the missed canal through intercanal communications
Dense invaginatus